 Português
Português English
English
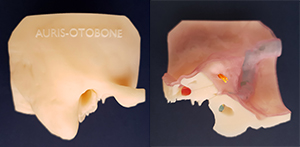 Auris-Otobone is an artificial temporal bone developed from a human CT. The current solution for training in any environment.
Auris-Otobone is an artificial temporal bone developed from a human CT. The current solution for training in any environment.
Developed and tested in the laboratories of the medicine faculties of the USP and the REPLICARE, Medicina 3D, produced with a special material with density similar to a biological bone.
HOW DID THE AURIS-OTOBONE ?
With difficulty in obtaining anotomical parts in corpses and with the increase in the number of specialists in educational institutes this is the ideal solution training.
Developed by the doctors, Ricardo Bento, Fernando Balsalobre, and Edson Leite Freitas (ENT) in partnership with the engineering and developing product team of REPLICARE, Medicina 3D.
AURIS-OTOBONE – DEVELOPMENTS IN SURGICAL TRAINING
The otobone is a faithful representation of the human temporal bone (mastoid) that enables medical training through surgical simulation, minimizing the use of cadaver parts.
Through patented technology jointly developed by REPLICARE, Medicina 3D, the Otorhinolaryngology Foundation and the Department of Otorhinolaryngology FMUSP, Our solution accurately reproduces the internal and external anatomical structures of the human temporal bone.
It was developed from a CT scan of a young adult, with no anatomical or pathological changes. Its design and manufacture aim to maintain anatomical fidelity and provide the closest possible experience to real dissection. Auris-Otobone is an alternative to the use of cadaverous pieces, facilitating the training of otorhinolaryngologists.
PROCEDURES THAT CAN BE TRAINED
Closed and open cavity tympanomastoidectomy
Posterior tympanotomy
Surgery for placement of anchored hearing aids
Cochlear implant surgery
Stapedotomy
Ossicular chain reconstructions
Facial nerve decompression
Petrosectomy
PRATICAL DISSECTION MANUAL – AURIS – OTOBONE
This piece was reconstructed from a high resolution CT scan of a adult patient with normal temporal bone.
- Please use masks and eye goggles;(for powder protect)
- We suggest the use of water irrigation during the dissection.
- There is no risk of infectious contamination since it is not made of biological material.
Materials required for dissection:
- A temporal bone holder that allows movement in multiple planes relative to the axis (there are several models in the market). In our site we have available the model developed by Prof. Ricardo Bento.
- A high speed surgical micro drill (of 35,000 rpm/min or more) with handpiece (straight and angled) and possibility of a two-way rotation.
- A surgical microscope with an objective of 250mm and angled or straight eyepiece of 10 or 12 X or magnifying glass.
- Alligator forceps and micro scissor.
- Surgeon’s preferential ear surgical set. It is essential to use a straight stylet, one with a 90-degree angle, a curette, and a elevator.
- Cutting burrs of various sizes.
Guidelines
The micro drill handpiece shall be preferably thin and held as a pencil by the dominant hand, being the suction tube held by the other hand.
The drilling shall be made with movements similar as in a painting with a delicate brush, parallel to the surface, without forcing the drill onto the bone, with intermittent force. The pressure must be firm and constant.
The drill’s side shall be used to cut the bone layer by layer in order to achieve minimum rough surfaces removing the mastoid air cells, localize and preserve the compact structures.
The drill’s velocity must be fast, because a slow velocity requires more force to cut the bone, with a greater chance of “sliding” to important structures. The drill must be kept clean from bone residues. Always use a small curette when there is a path to be explored rather than drilling it directly.
IDENTIFICATION OF EXTERNAL ANATOMICAL STRUCTURES (Please watch the movie in our site)
The temporal bone is divided into 5 distinct parts united by fissures:
- Squamous
- Mastoid
- Tympanic
- Styloid
- Petrous
external or lateral surface
- Zygomatic process
- Styloid process
- Glenoid fossa
- Tympanic bone
posterior or medial surface
- internal auditory canal (with the facial nerve (yellow) and cochlear and vestibular nerves(orange)
- dura mater of middle and posterior fossa
Posteior lateral semicircular cannal elevation.
Endolymphatic sac (red)
Sigmoid sinus (blue)
Superior surface
- petrous crest
- arcuate eminence (the superior semicircular canal projection in the middle fossa floor)
Tegmen timpani
Meatal Plan or surface (from the internal auditory meatus)
Inferior or base surface
- stylomastoid foramen, where the facial nerve emerges into the soft tissues of the neck (nerve stained in yellow)
- insertion of the digastric muscle on the mastoid (digastric groove)
- glenoid fossa, where the temporomandibular joint articulates
- zygomatic process anteriorly
- jugular fossa (blue)
- carotid canal (red)
- Jacobson canal opening (inferior tympanic nerve – branch of the IX cranial nerve)
- petrotympanic suture
- chorda tympani nerve passage opening (Huguier canal)
- Petrous apex
- Isthmus of Eustachian tube
Mastoidectomy and Atticotomy
Locate the external acoustic meatus (E.A.M.), the suprameatal spine (Henle’s spine), the timpanosquamous suture (Glazer notch) and the tympanomastoid suture.
Using a large round drill begin removing the cortex or the mastoid’s cortical in the angle formed by the intersection of an imaginary line parallel and inferior to the temporal line that divides the E.A.M. in the middle and another line that passes by the mastoid tip (mastoid eminence) making a 90 degrees angle with the temporal line. This point is posterior to the suprameatal spine (Henle’s spine) and is over the cribiform area of the mastoid. Go deeper in equal layers, remove all the cells.
Locate the following structures:
Note: The posterior wall of the E.A.M. shall be thinned as much as possible and, following it, follow superiorly toward the attic until the superior limit with the middle fossa, and inferiorly until the mastoid tip.
- external acoustic meatus (E.A.M.)
- suprameatal spine
- tympanosquamous suture
- tympanomastoid suture
- cribiform area
- mastoid tip
- sigmoid sinus (blue)
- sinodural angle
- digastric notch
- posterior wall of E.A.M.
- dura-mater of the middle fossa
- mastoid antrum
- incus
- lateral semicircular canal
With a small round drill, start drilling the superior attic region slowly, thinning the posterior wall of the E.A.M. between it and the middle fossa.
- zygomatic arch
- attic
- tympanic box
- malleus
- tegmen tympani
- posterior semicircular canal
- jugular bulb (blue)
- Fallopian canal
- dura-mater of the posterior fossa
Endolymphatic sac (red)
posterior tympanotomy, facial nerve and bone interposition
- facial nerve (yellow)
- stapes
- oval window
- round window
- cochlea
- cochleariform process
- pyramidal eminence
- Eustachian tube
- stylomastoid foramen
labyrinth removal and transmastoid exploration of the internal aucustic meatus
- vestibule
Facial nerve in the labyrinthine segment. And the genicular ganglion.
- internal acoustic meatus with facial nerve (yellow); vestibular nerves and cochlear nerve.
- internal carotid artery
It´s possible to practice stapedectomy, some auditory implants as cochlear implantR, VibrantR, BonebridgeR and PontoR and BahaR.
For further information, please contact:
FUNDAÇÃO OTORRINOLARINGOLOGIA
Phone: +55 11 3068 9855
E-mail: contato@otobone.com.br
Website: www.otobone.com